Hip Pain & Your Pelvic floor

Hip pain & your pelvic floor - what high achieving athletes Frustated with chronic hip pain need to consider.
Hip, groin, and or pelvic pain in sport can be due to a variety of causes- ranging from overuse injuries from repetitive movements in sports such as running, kicking, and jumping to limited mobility, hypermobility, muscle imbalances, or injury to connective tissue and ligamentous structures.
(Image used with permission from Pelvic Guru®, LLC www.pelvicglobal.com)
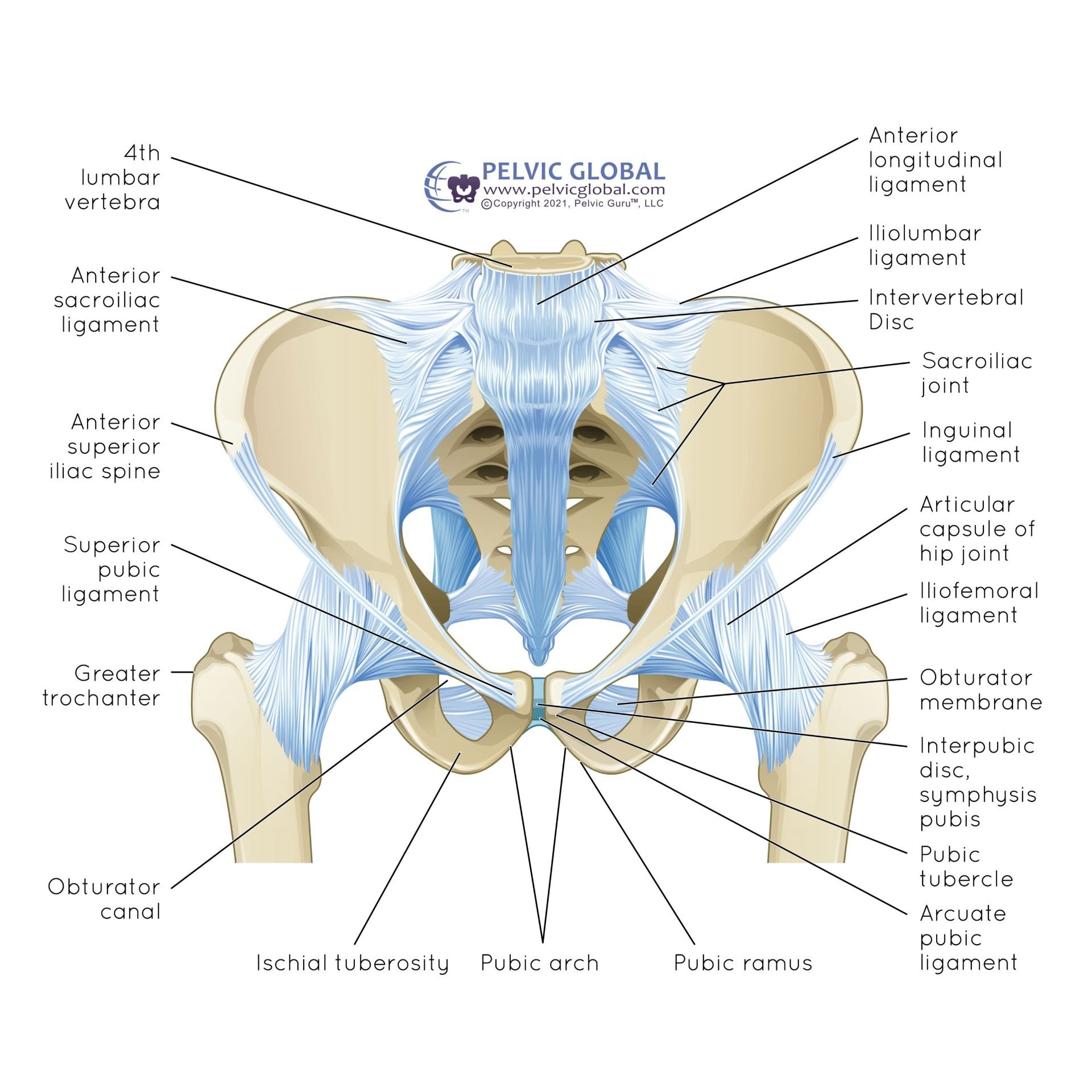
An underlooked potential primary or secondary source of hip pain is the pelvic floor musculature. The pelvic floor muscles live on the base of the pelvis with connections to the coccyx, pubic bone, sacrum, and fascial connections through the labrum to the femur. The role for the pelvic floor muscles is to support the pelvic organs (bladder, bowel, and uterus in females), control continence of bowel and bladder, allow elimination of urine and fecal matter, facilitate sexual function, in addition to contributing to trunk control.

(Image used with permission from Pelvic Guru®, LLC www.pelvicglobal.com)
Sharing bony structures with the pelvic floor is the hip joint which receives its support from the surrounding bony structures, ligaments, connective tissues and muscles. The hip is a ball and socket joint followed by the head of the femur which is the “ball” which rests in the “socket” which is the acetabulum of the pelvis.
A strong hip rotator needed for sport and that also provides support to the pelvic floor contents is the obturator internus. The Obturator internus has attachments to the ilium bones of the pelvis, the obturator membrane and the great trochanter of the femur sharing space with the piriformis muscle which originates on the front surface of the sacrum.

(Image used with permission from Pelvic Guru®, LLC www.pelvicglobal.com)
In dynamic sports such as running, the gluteals and adductor muscles are known work concoordinately to control the position of the femur while the pelvic floor muscles respond reflexively to control continence and support the hip concurrently through shared attachment sites. Common pelvic floor dysfunctions in sport include pelvic pain, urinary incontinence, and pelvic organ prolapse. Studies have shown that female runners who report urinary leakage also present with decreased hip abduction and rotation strength highlighting the interplay of the dynamic support needed at the hip in sport. For example, the prevalence of urinary leakage is 50% female weightlifters and 76% in female volleyball players, even affecting up to 33% elite female and male athletes participating in running sports, with incidence 5x higher in females.
While studies have discussed the role of the adductor muscle length and strength in the relation to groin pain, not many studies have looked at the integrated role of the pelvic floor muscles in individuals complaining of hip and groin pain. Furthermore, if a female athlete has concurrent low back pain inclusion of the pelvic floor muscles in the treatment plan is prudent as 95% of women with low back pain have been found to have pelvic floor muscle problem with majority of the pelvic floor dysfunction due to overactivity.
Personalized assessments with a pelvic floor physical therapist is key for athletes to have a comprehensive differential diagnosis of pelvic floor problems from hip, groin, or lumbar musculoskeletal conditions and for proper treatment to be prescribed. Just like major muscles of the hip or shoulder can have overactive and tight causing restricted movement around the joint, the pelvic floor muscles can present in a similar pattern- overactive and tight leading to decreased circulation and altered coordination patterns resulting in pain localized or in pain in a referral pattern and treatment for overactive muscles is not the same as a treatment for underactive or weak muscles.
Because the discussion of accidental bladder leakage or genital pain is considered taboo or individuals might be embarrassed to discuss, many athletes often underreport symptoms of pelvic floor dysfunction whereby developing chronic issues due to the delay of starting treatment. Comprehensive treatment of pelvic and hip pain for athletes not only should include a thorough training and sports injury history, but attention to pelvic floor function, hormonal, and nutritional status due to the unique interplay of these entities on female athletic performance.
At Radiance Physical Therapy, LLC, not only will you have a tailored treatment plan with a pelvic floor physical therapist knowledgable of the demands of your sport, using a collaborative approach to go from feeling frustrated and held back by pain to confidently finding long lasting relief of your persistent hip pain and clarity on how to keep running and stay active in the sport you love.
References
Donnelly et al. Sports Medicine & the Pelvic Floor. British Journal of Sports Medicine, 2023.
Tuttle, Lori J. et al. The Role of the Obturator Internus Muscle in Pelvic Floor Function. Journal of Women's Health Physical Therapy 40(1):p 15-19, January/April 2016.
Hartigan, Erin et al. Pelvic Floor Muscle Performance, Hip Mobility, and Hip Strength in Women With and Without Self-Reported Stress Urinary Incontinence. Journal of Women's Health Physical Therapy 43(4):p 160-170, October/December 2019.
Leitner et al 2016. Evaluation of pelvic floor muscle activity during running in continent and incontinent women: An exploratory study
Bo Kari, et al. Elite female athletes’ experiences of symptoms of pelvic floor dysfunction: a systematic review , Journal of Pelvic, Obstetric and Gynaecological Physiotherapy, Spring 2023, 132, 17–48
Rebullido, Tamara Rial PhD et al. Pelvic Floor Dysfunction in Female Athletes: Is Relative Energy Deficiency in Sport a Risk Factor?. Current Sports Medicine Reports 18(7):p 255-257, July 2019.
Bryd, Thomas. Hip Arthroscopy in Athletes Oper Tech Sports Med 13:24-36, 2005
Alonso-Fernández D, et al. Effects of Copenhagen Adduction Exercise on Muscle Architecture and Adductor Flexibility. Int J Environ Res Public Health. 2022 May 27;19(11):6563.
Dufour et al, 2018. Association between lumbopelvic pain and pelvic floor dysfunction in women: A cross sectional study, Musculoskeletal Science and Practice 34 (2018) 47–53
All Pelvic Guru images used with permission as a member of Pelvic Global